
Multi Frequency Vibrometry
Multi Frequency Vibrometry (MFV) is an objective medical examination method, used to support diagnosis of damage to Mechanoreceptors, Nerve fibers and Nerve trunks in the hands and feet, so-called Peripheral Sensory Neuropathy.
MFV measures and quantify the ability to feel and perceive vibrations applied to the skin, The method is specified in the ISO standard 13091-1/2.
Multi Frequency Vibrometry provides a reliable and a very early warning of the onset of sensory impairments due to incipient neuropathy or nerve entrapment, caused by, for example, diabetes, chemotherapy or or nerve entrapment, such as carpal tunnel syndrome
Research at Lund University and Skåne University Hospital in Malmö shows that MultiFrequency Vibrametry can detect changes significantly earlier than other methods
Research behind the method
Multi Frequency Vibrometry is developed by professors Göran Lundborg and Lars Dahlin et.al at the university hospital in Malmö and Lund. The method can be described as a hearing test on the skin since the method is strongly influenced by audiometry
A fingertip, or a point on the sole of the foot, is exposed to a controlled mechanical vibration of varying strength and frequency. The patient responds by pressing a response button when she/he can perceive a vibration in the skin and the result is recorded and stored in a Vibrogram.
Possibility to take preventive measures
Multi Frequency Vibrometry is an integral part of the VibroSense Meter II which can detect pre-symptomatic or subclinical changes. As an advantage, the instrument can also be used to follow the development of neurological changes (damage or healing) over time.This means that preventive measures can be put in place to prevent delay or mitigate permanent damage.
Several patient and occupational groups are at risk
Multi Frequency Vibrometry can be used in several contexts where neuropathy may occur, for example in diabetes, chemotherapy, vibration damage, alcoholism, drugs and more.
Sensory impairments often evolves slowly when working with vibrating tools where vibrations are transferred from the tool to fingers, hands and arms. Workers in vehicle workshops, on construction sites, in the engineering industry, with dental and foot care are at high risk of getting this type of damage.
Physiological measurement principle
The vibration sense is part of the neuro sensory system. In the skin there are a number of mechanoreceptors which are activated by different stimuli, including static pressure and vibrations. Different receptors react to different frequencies. The receptors are connected to fine nerve fibers that run together into so-called nerve trunks. Multi Frequency Vibrometry takes advantage of this fact, which gives the doctor valuable information at diagnosis
The vibration sensitivity deteriorates with age
The vibration sense has a maximum sensitivity between 200-250 Hz, which probably involves several types of receptors. The vibration sensitivity deteriorates with age, just like the hearing. In particular, the ability to perceive higher frequencies deteriorates.
The mechanoreceptors are connected to myelinated nerve fibres which are collected in larger nerve trunks. These lead up to the brain via various "connections" passing the spine. If a patient does not perceive a particular frequency, it may be due to several reasons, ranging from a thick fibre neuropathy in e.g. the foot or fingers to a nerve compression along path to the brain.
Measuring procedure
Automatic comparison with age and gender matched reference data
An examination of the sensitivity with VibroSense Meter II works in the same way as a hearing test. The VibroSense Meter II records objective Vibration Perception Thresholds (VPT) at different frequencies and compares them with the reference data from 1100 healthy subjects, age 8-70. Thus the comparison is also made with an automatic age- and gender matching. The latter is important, since the vibration perception capacity (as the hearing) deteriorates with age.
Fast and easy examination
During an examination, the patient first place the foot or a fingertip on a small "rod" which then starts vibrates with different intensity and frequency. The patient responds by pressing a response button (and holding it down) as long as she or he can perceive a vibration. The examination is fast (about 3-4 minutes per examined point) and very easy to perform.
Vibrogram disclose deviations
The result is recorded in a graphical curve, a Vibrogram, which shows whether the sensitivity is within a normal range or if there is a risk of incipient injury. A full examination with VibroSense Meter II includes measuring of two points per foot: under the big toe and under the little toe (metatarsal head I/V). Two fingers are examined on the hand (index finger and little finger. DIG II and V).
A questionnaire for different types of indications is integrated into the VSM PC software, which can be used to supplement the examination. The VibroSense Meter II software also contains multiple modes for screening examinations. Then a simplified and faster procedure is used.

Vibrogram
Reports neurological sensory status
VibroSense Meter II measures the ability to perceive fine tuned vibrations applied to the skin of the foot or hand, at up to seven different frequencies between 4 and 500 Hz. For each frequency, a Vibration Perception Threshold (VPT) is recorded. In the skin, there are various Mechano receptors which are actitvated within specific frequency ranges. Hence, it is not enough to just measure the sensitivity at one frequency to get an overall picture of the Neural Sensory Status.
Age and gender-related reference curve
During an examination with the VibroSense Meter II, a Vibrogram is recorded which usually has a characteristic shape. The Vibrogram is a graphic curve that shows the neuro sensory status (vibration sensation) in relation to an age- and gender-matched reference curve for healthy individuals.
An impaired sensitivity of vibration is associated with different changes to the shape of the Vibrogram curve.

Result reported in different units
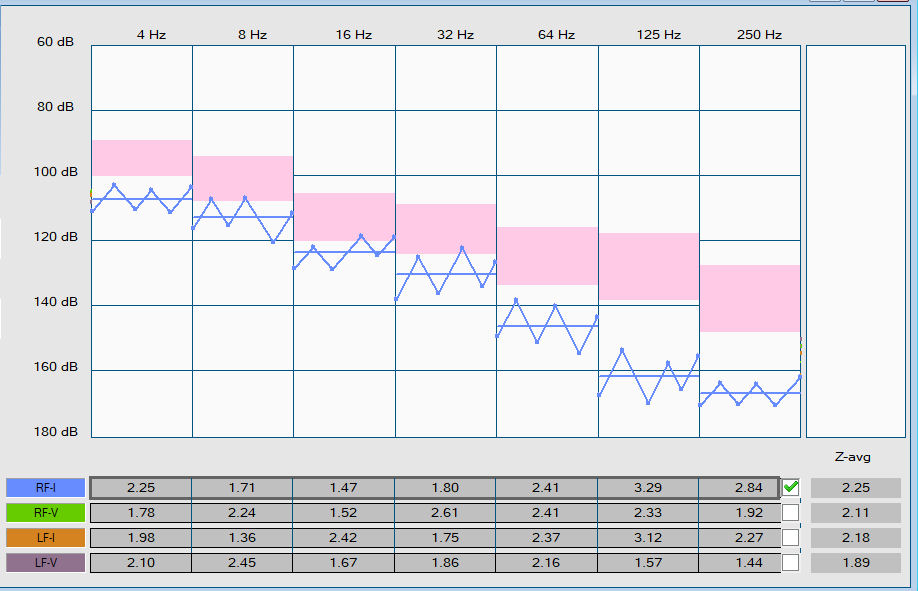
Impaired vibration sensitivity results in a visible change in the Vibrogram curve. In the Vibrogram, the patient's curve is shown in relation to an age-related reference curve (shaded pink area) on the screen. The patient's Vibrogram can therefore be directly compared against age-related normal values.
The result can be reported in two different units, i.e. Z-score or as threshold values in the unit dB. The Vibrogram shows directly whether the sensitivity is normal or whether there is a risk of incipient change or suspected damage. Click on the links to compare a normal curve (healthy person) with a curve with early changes (pathological outcome).
In normal cases, the measurement unit Z-score is used, but it is also possible to display the threshold value (VPT, Vibration Perception Threshold) in dB for each frequency. However, the threshold value does not say anything about how the result compares to a healthy person of the same age and gender
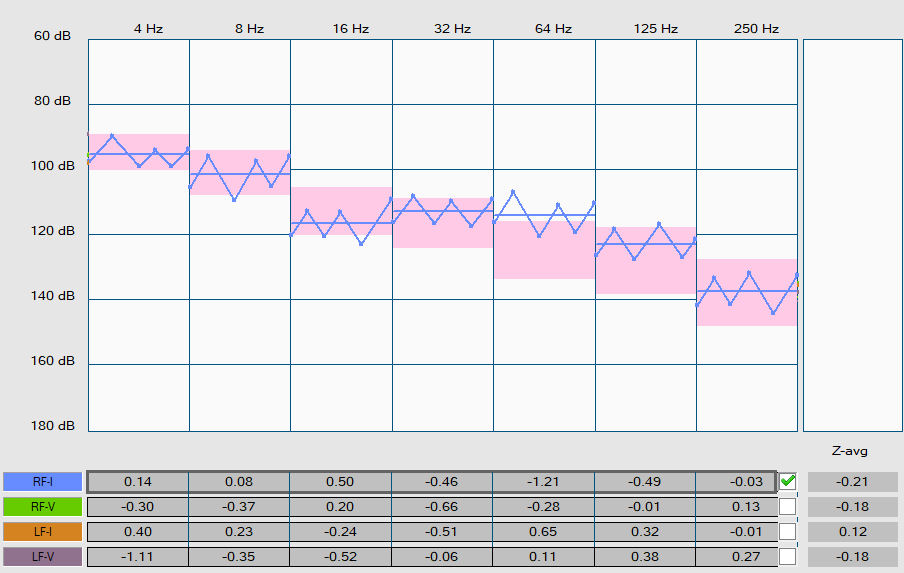
Z-Score and Z-avg
A Z-Score, as measured by the VibroSense Meter II. is a quantitative figure of how many standard deviations the threshold is positioned from the mean of the Gender- and age-matched normal range. Z-score is calculated for a single vibration threshold (VPT), i..e one for each frequency. The measure Z-score is a common term that is often used in research and development in medical technology and Pharma.
A Z-score = 0 indicates that the VPT is identical to the mean value in the reference data. A Z-score = 1.0 means that the measured VPT is one standard deviation higher than the mean value. Z-scores can be positive or negative.
As a rule of thumb, Z > 2 for a frequency should be interpreted as a pathological value in a Vibrogram. Z-score is also called Altman Z-score.
In addition to the Z-score for each individual vibration frequency, an index (average value) is calculated for several measured Z-scores. Currently there are two different indexes: Z-avg = Average value of 7 measured frequencies. Z-avgS = Average value of 3-4 measured frequencies used in foot or hand screening.
In general, cutoff values are defined as confidence intervals in relation to above mentioned data from healthy subjects.
The following general cut off values are recommended, defined as a mean value (Z-avg) of the Z-score for each examined frequency:
Z-avg < 1.7 ==> Normal value
1.7 ≤ Z-avg < 2.0 ==> Suspected impairment ( 95-97.5% confidence interval, single side)
2.0 ≤ Z-avg ==> Significant impairment ( 97.5% confidence interval, single side)
The ratio of the patient curve to the normal curve
Changes in the shape of the curve give an early indication of an incipient sensory disturbance. The curve is compared with an extensive Gender and age-matched normal data. It will therefore be possible to determine directly during the examination how the current patient curve relates to the normal curve.
Z-avg should be regarded as a quantitative average of the neural sensory function, which gives the doctor a quick indication of sensation status. In addition to the Z-avg, the appearance of the Vibrogram should also be analysed, because incipient sensory disturbances are visible early even if the Z-avg is below 1.7. See also the section "Interpreting Vibrograms" below.
Vibrogram Interpretation
Screening
With Screening, the VibroSense Meter system offers an examination that can quickly and effectively detect people who have an impairment or an increased risk of developing an injury. The goal is to quickly sort out all patients classified as normal to allow focus on those who are judged to have suspicious or significant abnormalities.
A classification of the result with a traffic light is included for two current available examinations i.e. the Diabetic Foot Screening and HAVS Screening. These classifications are based on extensive clinical data collected from people with diabetes and from people who are exposed to vibrations in their daily work.
Contact us for more information on how the results from screening can be interpreted.
Extended examination
An extended examination is recommended for in three cases:
1. When the result from a Screening (Diabetes or HAVS) is classified as Yellow or Red
2. Patients who with a suspected or with a pronounced neurosensory impairment in the foot/leg or fingers/arm.
3. Additional indication which may include neurosensory impairments
Depending on the clinical question, it is possible to examines up to two sites bilaterally on the foot or hand. An extended examination on the foot is performed at 7 frequencies from 4 – 250 Hz, under the big toe and little toe (metatarsal heads I and V) bilaterally, i.e. a total of up to 4 measurement points.
On the hand, an extended examination can be made on the index and little finger (Dig II and V), bilaterally, on 7 frequencies from 8 – 500 Hz.
Monitor the finger temperature
If the patient's hands are cold (finger temperature below 27 °C), this may result in high threshold values at 250 and 500 Hz without necessarily being signs of an impairment. It is therefore important to take the patient's temperature into account and redo the examination if the resuls looks odd.
The finger temperature is automatically recorded by the VibroSense Meter system, but the system allows an examination even if the patient's finger temperature is low.
When examining the foot, the temperature is less important, but the temperature is still recorded and saved automatically before an examination.
Outcome from four measuring sites on the hand or foot
An extended examination on the hand or foot can provide valuable information with so-called differential diagnostics. In normal cases, the vibration sensitivity is the same on the right and left side of the body (hand or foot). In a Vibrogram, it's possible to detect if there are differences between the right and left sides or between two measurement points on a hand or a foot.
Nerve Entrapment
The sensitivity in the index and little finger reflects the function of the medianus and the ulnaris nerve, respectively. The outcome for all four fingers may tell a lot about the cause of the sensory disorder. A vibration injury usually renders a pathological outcome for several, usually in all four fingers.
A Carpal Tunnel Syndrome in one hand normally results in a pathological Vibrogram curve for the index finger (Dig II), but with normal outcome for the other fingers.
For the foot, a measured difference between the right and left foot can be a sign of nerve entrapment in the Sciatic nerve.

